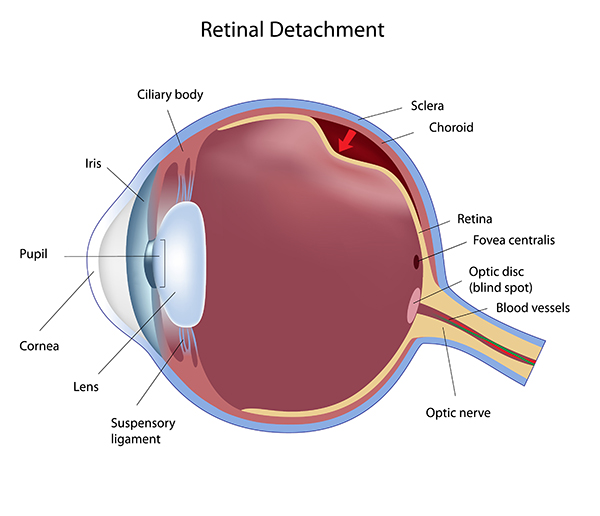
Retinal detachment is a disorder of the eye in which the retina separates from its underlying layer of support tissue. Initial detachment may be localized, but without rapid treatment the entire retina may detach, leading to vision loss and blindness. Retinal Detachment is a medical emergency.
The retina is a thin layer of light sensitive tissue on the back wall of the eye. The optical system of the eye focuses light on the retina much like light is focused on the film in a camera. The retina translates that focused image into neural impulses and sends them to the brain via the optic nerve. Occasionally, posterior vitreous detachment, injury or trauma to the eye or head may cause a small tear in the retina. The tear allows vitreous fluid to seep through it under the retina, and peel it away like a bubble in wallpaper.
Eye condition: retinal detachment
A retinal detachment is commonly preceded by a posterior vitreous detachment which gives rise to these symptoms:
flashes of light (photopsia) – very brief in the extreme peripheral (outside of center) part of vision
a sudden dramatic increase in the number of floaters
a ring of floaters or hairs just to the temporal side of the central vision
a slight feeling of heaviness in the eye
Although most posterior vitreous detachments do not progress to retinal detachments, those that do produce the following symptoms:
a dense shadow that starts in the peripheral vision and slowly progresses towards the central vision
the impression that a veil or curtain was drawn over the field of vision
straight lines (scale, edge of the wall, road, etc.) that suddenly appear curved (positive Amsler grid test)
central visual loss
(None of this is to be confused with the broken retina which is generally the tearing of muscle and nerve behind the eye)
Treatment
There are several methods of treating a detached retina which all depend on finding and closing the breaks which have formed in the retina.
Cryopexy and Laser Photocoagulation
Cryotherapy (freezing) or laser photocoagulation are occasionally used alone to wall off a small area of retinal detachment so that the detachment does not spread.
Scleral buckle surgery
Scleral buckle surgery is an established treatment in which the eye surgeon sews one or more silicone bands (bands, tyres) to the sclera (the white outer coat of the eyeball). The bands push the wall of the eye inward against the retinal hole, closing the break or reducing fluid flow through it and reducing the effect of vitreous traction thereby allowing the retina to re-attach. Cryotherapy (freezing) is applied around retinal breaks prior to placing the buckle. Often subretinal fluid is drained as part of the buckling procedure. The buckle remains in situ. The most common side effect of a scleral operation is myopic shift. That is, the operated eye will be more short sighted after the operation. Radial scleral buckle is indicated to U-shaped tears or Fishmouth tears and posterior breaks. Circumferential scleral buckle indicated to multiple breaks, anterior breaks and wide breaks. Encircling buckles indicated to breaks more than 2 quadrant of retinal area, lattice degeration located on more than 2 quadrant of retinal area, undetectable breaks, and proliferative vitreous retinopathy.
Pneumatic retinopexy
This operation is generally performed in the doctor’s office under local anesthesia. It is another method of repairing a retinal detachment in which a gas bubble (SF6 or C3F8 gas) is injected into the eye after which laser or freezing treatment is applied to the retinal hole. The patient’s head is then positioned so that the bubble rests against the retinal hole. Patients may have to keep their heads tilted for several days to keep the gas bubble in contact with the retinal hole. The surface tension of the air/water interface seals the hole in the retina, and allows the retinal pigment epithelium to pump the subretinal space dry and suck the retina back into place. This strict positioning requirement makes the treatment of the retinal holes and detachments that occurs in the lower part of the eyeball impractical. This procedure is usually combined with cryopexy or laser photocoagulation.
Vitrectomy
Vitrectomy is an increasingly used treatment for retinal detachment. It involves the removal of the vitreous gel and is usually combined with filling the eye with either a gas bubble (SF6 or C3F8 gas) or silicon oil. Advantages of using gas in this operation is that there is no myopic shift after the operation and gas is absorbed within a few weeks. Silicon oil (PDMS), if filled needs to removed after a period of 2–8 months depending on surgeon’s preference. Silicon oil is more commonly used in cases associated with proliferative vitreo-retinopathy (PVR). A disadvantage is that a vitrectomy always leads to more rapid progression of a cataract in the operated eye. In many places vitrectomy is the most commonly performed operation for the treatment of retinal detachment.